The authors of this article published in American Heart Journal would like to thank Professor Gian Luca Di Tanna for his biostatistical assistance.
Background
Despite high blood pressure being the leading preventable risk factor for death, only 1 in 3 patients achieve target blood pressure control. Key contributors to this problem are clinical inertia and uncertainties in relying on clinic blood pressure measurements to make treatment decisions.
Methods
The NEXTGEN-BP open-label, multicenter, randomized controlled trial will investigate the efficacy, safety, acceptability and cost-effectiveness of a wearable blood pressure monitor-based care strategy for the treatment of hypertension, compared to usual care, in lowering clinic blood pressure over 12 months. NEXTGEN-BP will enroll 600 adults with high blood pressure, treated with 0 to 2 antihypertensive medications. Participants attending primary care practices in Australia will be randomized 1:1 to the intervention of a wearable-based remote care strategy or to usual care. Participants in the intervention arm will undergo continuous blood pressure monitoring using a wrist-wearable cuffless device (Aktiia, Switzerland) and participate in 2 telehealth consultations with their primary care practitioner (general practitioner [GP]) at months 1 and 2. Antihypertensive medication will be up-titrated by the primary care practitioner at the time of telehealth consults should the percentage of daytime blood pressure at target over the past week be <90%, if clinically tolerated. Participants in the usual care arm will have primary care consultations according to usual practice. The primary outcome is the difference between intervention and control in change in clinic systolic blood pressure from baseline to 12 months. Secondary outcomes will be assessed at month 3 and month 12, and include acceptability to patients and practitioners, cost-effectiveness, safety, medication adherence and patient engagement.
Conclusions
NEXTGEN-BP will provide evidence for the effectiveness and safety of a new paradigm of wearable cuffless monitoring in the management of high blood pressure in primary care.
Burden of uncontrolled blood pressure and role of clinical inertia
High blood pressure (BP) is the leading reversible risk factor for mortality globally.1,2 Better BP control could save more lives than any other single treatment intervention.3 However achievement of target BP control remains a major global challenge.4., 5., 6., 7. In Australia, BP control rates have stagnated since 2011 at 32%,4,8 comparing poorly to countries such as Canada or the United States with control rates of 65% and 48%, respectively.9,10 Underlying this suboptimal control is clinical treatment inertia,11 ie, clinicians do not initiate or intensify therapy in a patient who has not achieved therapeutic goal. Treatment inertia is a complex phenomenon,12 but it is frequently driven by uncertainty around “usual” BP levels for both a treating clinician and the patient,13 leading to a reluctance by both parties to initiate or intensify pharmacological treatment. Very often there will be a tendency to remeasure high BP levels to check, and then to “believe” subsequent lower measures.
Novel approaches are therefore needed to overcome inadequacies in clinic BP monitoring, treatment assessment, and therapeutic inertia. Such a strategy would include a substantially increased number of BP readings to account for the normal fluctuation in BP levels, patient-centered decision-making approaches for treatment adjustment, and patient engagement.14
Rationale for a remote decision support strategy based on wearable blood pressure monitoring
The NEXTGEN-BP open-label, multicenter, randomized controlled trial will investigate the efficacy, safety, acceptability, and cost-effectiveness of a multifaceted remote wearable out-of-office BP -based care strategy for the treatment of hypertension compared to usual care, in lowering clinic BP over 12 months. The COVID-19 pandemic has led to broader implementation of remote-based care including telehealth and increased remote monitoring. Home remote BP monitoring through cuffless monitoring via the Aktiia device (described below) will be combined with telehealth visits by the primary care practitioner (general practitioner [GP]). A decision-support aid to interpret multiple BP readings obtained through continued cuffless monitoring will be used to simplify the prescription of antihypertensive therapies and to overcome therapeutic inertia in primary care.
To overcome the challenges of “snapshot” clinic BP readings and to obtain out-of-office BP measurement, cuffless wristband wearable technologies have been incorporated into a remote wearable BP-based care strategy. Samsung, Fitbit and Apple have filed several patents for cuffless BP monitoring,15 and in Australia we have found more than 530 cuffless wristband BP devices on the market.16 These devices typically use photoplethysmographic signals to calculate BP using pulse wave analysis combined with appropriate algorithms. The Aktiia device (Aktiia SA, Switzerland, Supplemental Figure 1) requires a monthly calibration by the participant with upper-arm cuff BP. 17., 18., 19 The device provides automated BP measures for weeks at a time, without using a cuff. The device thus provides a long-term BP profile,20 and features such as long-term battery life and automated measurements without cuff disturbance,21,22 contributing to patients’ preference for cuffless BP monitoring over traditional 24-hour BP monitoring.22 The Aktiia device enables the user to access BP data through a mobile phone app that uploads the data via Bluetooth from the wrist-band. In this trial, the primary care practitioner will have access to a single measure that captures hundreds of data points—namely the % of daytime BPs at target (<135/85 mmHg) during the past week. This will allow the primary care practitioner and patient to make therapeutic decisions based on longer-term BP control (instead of relying on single snapshot clinic BP values). This aligns well with mounting evidence on the substantial survival benefits of consistent BP control over time.23, 24., 25. On a continuum, the time that BP is within the target range is significantly associated with a reduction in mortality23 and major cardiovascular events.24,25
In 2022 the European Society of Hypertension published a consensus statement recommending against the use of cuffless BP devices until accuracy and clinical usefulness have been established.26 In the absence of an appropriate ISO protocol (under development) to validate cuffless devices,26 the Aktiia device was validated using the ISO validation criteria for traditional cuff-based devices.17., 18., 19,27 It is approved and available in Europe (CE Mark Class IIa medical device) and approved in Australia (approved by the Therapeutic Goods of Australia (TGA)). We recently reported that when comparing the Aktiia device with cuff-based ambulatory monitoring, the Aktiia compared well for daytime BP values but not for nighttime.28 For this trial, decision-making will therefore be based on daytime BP readings after recent calibration. It is anticipated that in coming years, more validated wearable BP devices will be brought to market with due implications on primary care practice.
Objectives
The NEXTGEN-BP randomized trial is an investigator initiated and conducted trial sponsored by The George Institute for Global Health, Sydney, Australia. The primary aim is to assess in adults with hypertension, the efficacy of a remote wearable BP-based care strategy to reduce office BP in primary care over 12 months, compared to usual care. The secondary aims are to determine if this remote wearable BP-based care strategy is acceptable to patients and primary care practitioners through process evaluation; cost-effective; improves medication adherence; improves patient engagement; is safe, compared to usual care. We hypothesize that the remote wearable BP-based care strategy will be superior to usual care in terms of efficacy in BP reduction, acceptability to patients and primary care practitioners, and cost-effectiveness.
Methods and analysis
Trial design
We will conduct a 2-arm open-label randomized multicenter trial comparing a remote wearable BP-based care strategy for the treatment of hypertension, with usual care over 12 months (Figure 1). The duration of a 12 month intervention for both groups will enable assessment of the sustained effects of the strategy, and aligns with similar international trials on self-monitoring of BP in primary care.29,30 The design of this trial is open-label and will require 3 mandatory in-person study visits for both arms—at enrolment and at months 3 and 12, where the trial staff will capture any differences in clinic BP, medication prescriptions, adherence to medication, visit frequency and adverse events. The trial will be overseen by the Steering Committee (Supplement 1).
Figure 1. Study design

Participants
Inclusion Criteria. The trial will recruit male and female participants from general practices and outpatient clinics who meet the following criteria: (1) provide signed or electronic consent to participate in the trial; (2) aged ≥18 years; (3) average clinic seated mean systolic BP ≥140 and/or diastolic BP ≥ 90 mmHg, treated or untreated; or documented history of hypertension in the last 3 months (clinic ≥ 140/90 mmHg or home ≥ 135/85 mmHg); (4) willing to self-monitor BP; (5) own a compatible smartphone and ability to use it; (6) access to an internet connection to allow primary care practitioner telehealth consultations; (7) the patient is deemed eligible for the treatment protocol by the primary care practitioner.
Exclusion Criteria. Participants will be excluded if they are taking 3 or more BP-lowering drugs; the participant’s responsible primary care provider or other responsible physician deems that they are not suitable for remote management including use of wearable BP device, reporting of symptoms, and following electronic script-based titration steps; unable to complete trial procedures including cuffless BP monitoring; planned overseas travel in the first 30 days of joining the trial and if planning to travel for longer than 6 months during the trial period; primary care practitioner deems participant unsuitable to switch current antihypertensive therapy or a definite indication for combination therapy; currently pregnant; participation in a concurrent clinical trial of an investigational medicinal product; concomitant illness, physical impairment, psychiatric condition or cognitive impairment which in the opinion of the trial team/primary care physician could interfere with the conduct of the trial including outcome assessments.
Setting, location, and recruitment
Trial participants will be recruited from community general practices that provide hypertension care throughout Australia. The study staff will screen eligible participants using the protocol-defined inclusion and exclusion criteria described to identify a group of eligible people and obtain informed consent. Primary care practices will conduct audits to identify potentially eligible participants. Potential participants referred to or who contact the study staff directly will undergo screening to determine eligibility to the trial using the criteria described. Initial screening activities will include a brief verbal assessment of medical history, including hypertension history and current medications. Eligible participants will be provided a participant information sheet by the study staff and will be invited to read and contemplate the information prior to making a decision about involvement. Full informed consent will be obtained.
Study treatment
Intervention: a remote wearable BP-based care strategy
The intervention involves a multifaceted strategy designed to address treatment inertia in a remote care model. It firstly includes a clinical decision-making tool for primary care practitioners based on hundreds of automated BP readings generated over time by the Aktiia wrist-worn cuffless wearable BP device. Secondly, it includes mandatory primary care practitioner telehealth consultations (video or phone) at months 1 and 2 (Table I). Thirdly, it includes participant access to the Aktiia phone application to view blood pressures, and thus facilitate increased engagement.
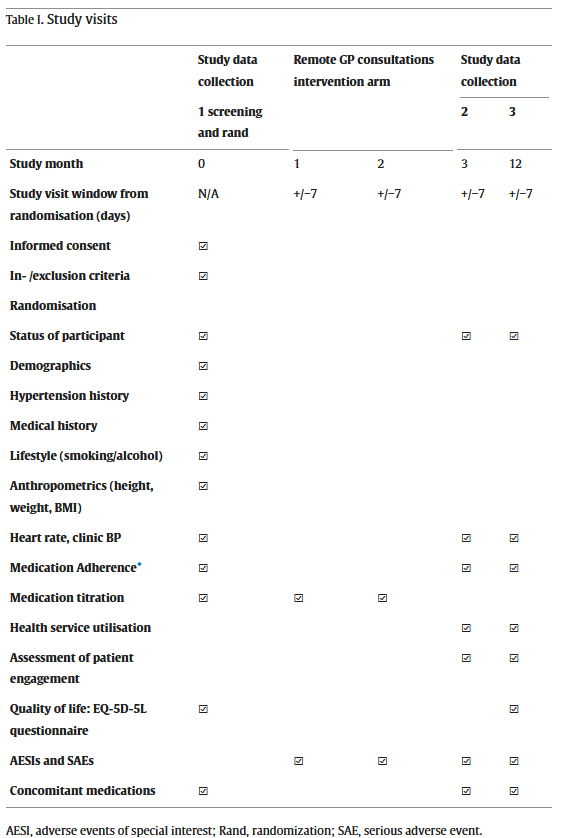
AESI, adverse events of special interest; Rand, randomization; SAE, serious adverse event.⁎
Apart from assessing adherence through the ARMS-7 questionnaire, participant consent will be obtained to access Pharmaceutical Benefit Scheme dispensing data.
To manage the challenge of interpreting hundreds of BP readings in primary care, the Aktiia device automatically generates a single number, to be used for clinical decision-making. This is the % of daytime BP values below the target of 135/85 mmHg over the past week (these are guidelines cut-offs for both daytime ambulatory BP and home BP).31., 32., 33. This single percentage value will replace clinic BP for clinical decision-making in the intervention group.
The clinical decision-making tool: Prior to each of the 2 telemonitoring patient visits at months 1 and 2, the percentage of daytime BPs at target over the past week will be provided by the study coordinating team to the participant’s responsible primary care provider through fax or email. The use of clinic BP will not be recommended. Patients will have continued access to their BP values shown on the Aktiia app on their smartphone (Figure 2). This will allow for discussion with their primary care practitioner and shared decision-making. The percentage of BPs at target will serve as a trigger to guide titration, aiming to achieve ≥90% of BP at target.23, 24., 25.
Figure 2. Aktiia mobile phone application and blood pressure titration strategy.
The following mandatory uptitration steps will be communicated to the primary care practitioner if <90% of BPs are at target and the patient is not reporting symptoms of hypotension (Figure 2). If the patient uses:
- (i)No medication—then start monotherapy;
- (ii)1 medication—add 1 medication;
- (iii)2 medications—double both doses (or add 1 medication);
- (iv)3 medications—ensure medications are at maximum dose or add spironolactone.
Down-titration or alternative antihypertensive medications may be required depending on participant symptoms. In the usual care group, BP therapy will be initiated or up-titrated as per the treating primary care practitioner’s discretion.
Study procedures
There are 3 mandatory study visits (Figure 1, Table I) to collect clinical data at baseline, 3 months and 12 months. The frequency, timing and content of all other in-person primary care practitioner visits are not determined by the trial and will be according to usual practice and primary care practitioner discretion. To assess all participant visit attendances and prescribing, consent will be obtained to access Medicare Benefits Schedule (MBS) and Prescription Benefits Scheme (PBS) data.
In the intervention arm, the study staff will provide training to fit the Aktiia device to the participant (Supplement 2) and calibrate the device monthly. Participants will have 2 remote visits with the primary care practitioner. Participants will be reminded to wear the Aktiia daily for at least 1 week prior to the remote visit. The coordinating team will provide the percentage BP at target over the past week to the primary care practitioner prior to the visit. The participant will have continued access to their BP readings through their Aktiia smartphone app. Based on the clinical decision-support tool (Figure 2), and during the 2 remote visits, the primary care practitioner will titrate BP therapy through electronic prescriptions.
Outcomes
The primary outcome is difference in change in clinic systolic BP from baseline to 12 months between intervention and control (mmHg) (Table II). Secondary outcomes include (1) Efficacy: Net difference in change in clinic BP from baseline to 3 and 12 months; Clinic BP control (%), achieving <140/90 mmHg at 3 and 12 months; Time at clinic BP target over 12 months; (2) Cost-effectiveness: Average total cost per patient achieving BP control, cost per quality-adjusted life year (QALY); (3) Engagement: Adherence (self-reported and through Pharmaceutical Benefits Scheme prescription fills); Visit attendance (through Medicare Benefit Schedule data); compliance with the intervention (continued use of wearable BP device based on data collected by the wearable device on data synchronization with the app); acceptability to patients and primary care practitioners; Patient activation; (4) Safety: incidence of adverse effects leading to treatment withdrawal (Supplement 3).
Table II. Primary and secondary outcomes for the NEXTGEN-BP trial
| Primary outcome | |
|---|---|
| Efficacy | •Difference in change in clinic systolic BP from baseline to 12 months (mmHg) |
| Secondary outcomes | |
| Efficacy | •Net difference in change in clinic BP from baseline to 3 and 12 months•Clinic BP control (%), achieving <140/90 mmHg at 3 and 12 months•Time at clinic BP target over 12 months |
| Cost-effectiveness | •Average total cost per patient achieving BP control, $/Quality-adjusted life year (QALY) |
| Engagement | •Medication adherence (self-reported measures and through Pharmaceutical Benefits Scheme prescription fills)•Visit attendance (through Medicare Benefit Schedule data; access)•Compliance with the intervention (continued use of wearable BP device)•Acceptability to patients and primary care practitioners•Patient activation; |
| Safety | •Incidence of adverse effects leading to treatment withdrawal |
Independent study personnel (blinded to patient allocation) will perform attended clinic BP measurements in a quiet room while the participant is in the seated position and in triplicate according to standardized procedures in practice guidelines using a validated upper-arm cuff oscillometric device (Microlife WatchBP Office device)34,31 We will use the average of the second and third BP reading.
Sample size
Assuming a common standard deviation of 17 mmHg35 of office systolic BP and an alpha of 0.05 using a 2-sided 2-sample equal-variance t-test, the study will have 90% power to detect a 5 mmHg between group difference in clinic systolic BP with 244 participants in each group. Allowing for a drop-out rate of 15%,35 the estimated total sample size is 576 participants (target n = 600). This sample size will also allow us to detect a difference of ∼15% in time at BP target (defined as % of time at target BP) with a power of 89% and at an alpha adjusted for multiplicity at 0.025. There will be a formal interim power review after approximately 100 patients have reached the primary endpoint. This assessment will be based on blinded data only and will utilize ANCOVA-based power calculations, which are more closely aligned with the final statistical analysis approach but also require additional modelling assumptions.
Randomization and allocation
This is an open-label, blinded end-point trial. Participants will be randomly assigned to either intervention or usual care group with a 1:1 allocation as per computer generated randomization schedule stratified by site using permuted blocks. Allocation concealment is maintained because only the unblinded statistician and unblinded data manager have access to the randomization list and allocation within the database. To reduce predictability of a random sequence, details of any planned restriction (eg, blocking) should be provided in a separate document that is unavailable to those who enroll participants or assign interventions. All participants and most of the study staff will be aware of the intervention as allocated. The outcome will be blinded, namely all follow-up measures will be conducted by study staff using about automated equipment who will remain blinded to treatment allocation.
Economic evaluation
We will evaluate within-trial and modelled long-term cost-effectiveness. Cost of the intervention compared to usual care will be based on the costs of cuffless BP devices, medication, number and costs of visits, and training. In-trial cost-effectiveness will be measured as cost per participant achieving BP control at 12 months. We will also use a decision-analytic model to simulate long-term cardiovascular outcomes, quality-of-life adjusted survival, and costs. In the modelled analysis, cost-effectiveness will be calculated in terms of incremental cost per QALY gained. We will request data from the Medicare Benefits Schedule (MBS) and the Pharmaceutical Benefits Scheme (PBS). MBS data will be accessed to determine the impact of the intervention on the use of healthcare visits and investigations—which will be an important component of the economic evaluation. PBS data will be accessed to determine blood pressure lowering medication information on prescriptions and refills.
Process evaluation
The process evaluation will collect quantitative and qualitative data to understand for whom, how and why our intervention resulted in the variation of outcomes. The evaluation will be informed by the UK Medical Research Council process evaluation guidance and an implementation research logic model36 outlining the contextual determinants, intervention, implementation strategies, mechanisms and implementation outcomes of reach, acceptability, appropriateness, and sustainability of the remote wearable BP-based strategy that spans patient and provider motivation, behavior and their interactions, and patient clinical outcomes.36 Sources include routinely collected trial data (eg, recruitment logs, app views by participants), secondary outcomes (eg, adherence, activation), and semistructured interviews with patients and primary care practitioners.
Trial participants (approx. n = 30) and health care providers (approx. n = 15-20) will be recruited using maximum variation purposive sampling in the usual care versus intervention arm, reflecting geographical location, age and sex diversity, knowledge, attitude, and behavior towards the wearable BP-based strategy. An implementation science framework that focuses on reasons for adoption, abandonment, scale up, spread and sustainability (NASSS) of health and care technologies will guide the development of the interview guides and analysis.37 For example, questions will focus on the perceived value of the intervention across patient, provider, and policy levels (eg, implementation costs and MBS), and reasons for its adoption. Findings will be fed back iteratively to the trial operations team to optimize trial implementation (eg, strategies to overcome identified barriers to remote prescription across different settings).
Statistical methods
All analyses will be performed on an intention-to-treat basis by investigators blinded to patient allocation. Baseline characteristics by the group will be compared using descriptive analyses. The primary outcome of difference in change in clinic systolic BP from baseline to 12 months will be estimated by a hierarchical linear model (mixed model repeated measures) with fixed effects for treatment group, time (clinic visit), treatment by time (clinic visit) interaction, baseline clinic systolic BP, and allowing for a random-effect at site level. Other continuous outcomes of difference in change in BP will also be estimated by the modelling approach used for the primary outcome. The proportion of participants achieving target BP at months 3 and 12 will be summarized descriptively as well as analyzed using a hierarchical log-binomial model with the treatment group as a fixed effect and the trial site as a random effect. Other binary outcomes of efficacy and safety will be analyzed similarly as the proportion of participants achieving target BP. A detailed statistical analysis plan will be developed and made publicly available prior to the final data-lock.
Data monitoring
An independent Data and Safety Monitoring Board (DSMB) will review the safety, ethics and outcomes of the trial. Their roles include monitoring blinded response variables and safety outcomes for potential harmful effects to ensure safety monitoring and provide reports to the Steering Committee on recommendations to continue or temporarily halt recruitment to the trial. The DSMB will be governed by a charter that will outline their responsibilities, procedures and confidentiality.
Trial management, funding, and sponsorship
The trial conduct is overseen by a Steering Committee (Supplement 1). The central coordinating center ensures implementation of the study according to the protocol, timelines, and recruitment targets. We use an electronic data management system incorporating study checks and omissions. This trial is funded by a Primary Health Care Research grant from the Medical Research Future Fund of Australia (Application ID 2017098). Investigators also received support from the NHMRC program and investigator fellowships to enable the study (see Funding statement).
Trial registration, human research ethics, and dissemination plan
The trial has received approval from the University of New South Wales relevant ethics committee (HC220617) and has been registered with the Australia New Zealand Clinical Trial Registry (ACTRN12622001583730).
The main trial results will be published in the name of the NEXTGEN-BP Investigators. The authors are solely responsible for the design and conduct of this study, all study analyses, the drafting and editing of the paper and its final contents. Publication authors must meet the International Committee of Medical Journal Editors guidelines for authorship. Trial findings will be presented at national and international meetings. Data will be made available through data access agreements established following approval through the Steering Committee. Trial data will not be publicly released or placed into an open-access repository. Trial data will be held by the George Institute for Global Health for a minimum period of 15 years (or longer if required by applicable regulatory authorities).
Discussion
This study will be the first large-scale randomized controlled trial to examine the application of the next generation of cuffless BP wearables embedded into a complex intervention in clinical practice. Not only will the trial evaluate the utility of wearable technology in clinical practice, but more importantly the ability of a remote decision support strategy based on wearable BP to change prescriber and patient behaviors to reduce treatment inertia. A constraint of our trial is that we will only use daytime BP due to the technological limitations of current cuffless devices.28 This approach has many potential theoretical benefits, including greater efficacy, improved patient engagement and medication adherence, and decreased costs. A meta-analysis by Tucker et al. demonstrated that traditional self-monitoring of BP at home with cointerventions (such as systematic medication titration by doctors, pharmacists, or patients; education; or lifestyle counselling) resulted in a 6 mmHg reduction in systolic BP, compared to usual care at 12 months.38 If this new intervention demonstrates a 5 to 10 mmHg additional BP reduction compared to that conferred by usual care, such a difference could translate into an additional 15% to 20% reduction in cardiovascular events.39
If the intervention tested here is proven to be safe and effective, the trial may provide policy-relevant evidence for a scalable new treatment strategy that could improve outcomes for patients with hypertension in clinical practice. By collaborating with treating clinicians and consumers as chief investigators, we ensure that the intervention will be readily and rapidly translatable into practice if successful. The Aktiia device is already available for purchase in Europe and the UK, and although cuffless BP monitoring remains a contentious topic, many other accuracy-validated BP wearable devices are anticipated in the future. The results of the current trial would stimulate further development of such technologies if the results were favorable. Results are also likely to impact clinical practice guidelines in Australia and internationally.
Conclusion
The proposed novel cuffless BP-based care strategy has the potential for major impact on current poor rates of BP control in Australia and globally. The NEXTGEN-BP trial will provide direct evidence on efficacy, acceptability and cost-effectiveness in a large-scale randomized controlled trial. If the intervention tested in this trial is proven to be safe and effective, the results could transform the approach to BP management, with benefits in routine clinical practice. The results of the current trial could be a paradigm changer in the clinical management of hypertension.
Author contributions
Sonali R Gnanenthiran and Aletta E Schutte were involved in the planning and writing of this manuscript. All other authors reviewed the manuscript and provided intellectual input.
Disclosures
JES is principal investigator of a National Health and Medical Research Council partnership grant (S0026615) on cardiovascular disease risk assessment; among the partners listed on that grant is a medical technology company that manufactures a central BP monitor. AES received speaker honoraria from device manufacturers, Omron and Aktiia. GSS received consulting and lecture fees from several manufacturers for developing blood pressure measuring technologies.
Funding
This trial is supported by a Primary Health Care Research grant from the Medical Research Future Fund of Australia (Application ID 2017098). Aletta E Schutte is supported by a NHMRC Leadership Investigator Grant (Application ID 2017504). Sonali R Gnanenthiran is supported by a Heart Foundation postdoctoral fellowship. Anushka Patel is supported by a NHMRC Leadership Investigator Grant (Application ID 2016801).